Fertility Basics
Amatoritsero Olumami-Oyibo ·
12 min read


FERTILITY EDUCATION
Medical information, not personal medical advice This guide provides general fertility education. Your symptoms, age, medical history, partner or donor sperm results and personal goals all affect which tests and treatments may be appropriate. Speak to a your clinician about your individual circumstances. |
|---|
In this guide
What female infertility means
What needs to happen for pregnancy
Common causes, including ovulation disorders, endometriosis and tubal factors
Symptoms and warning signs
When to seek fertility support
How female fertility is assessed
How treatment may help
Emotional wellbeing and frequently asked questions
Oocyt clinical principle A diagnosis is not a judgement about your body, and a test result is not a prediction of your future. Good fertility care connects the findings, your priorities and the safest next step. |
|---|
Why trust this guide?
This resource has been curated using current guidance from the World Health Organization, NICE, NHS and the American Society for Reproductive Medicine. It prioritises clear language, realistic expectations and the least invasive appropriate investigation first. [1-5]

What is female infertility?
Infertility is a condition of the reproductive system in which pregnancy has not been achieved after a period of regular unprotected intercourse or when a known condition is already affecting the ability to conceive. The World Health Organization commonly uses 12 months as the definition. [1]
In UK practice, NICE recommends further assessment after 1 year of unprotected intercourse when there is no known cause. It recommends referral at presentation when the person trying to become pregnant is aged 36 or over, or when either partner has a known or suspected fertility factor. [2]
Important Female infertility does not necessarily mean pregnancy is impossible. Some causes can be treated, some can be worked around with assisted conception, and some people conceive while investigations are ongoing. |
|---|
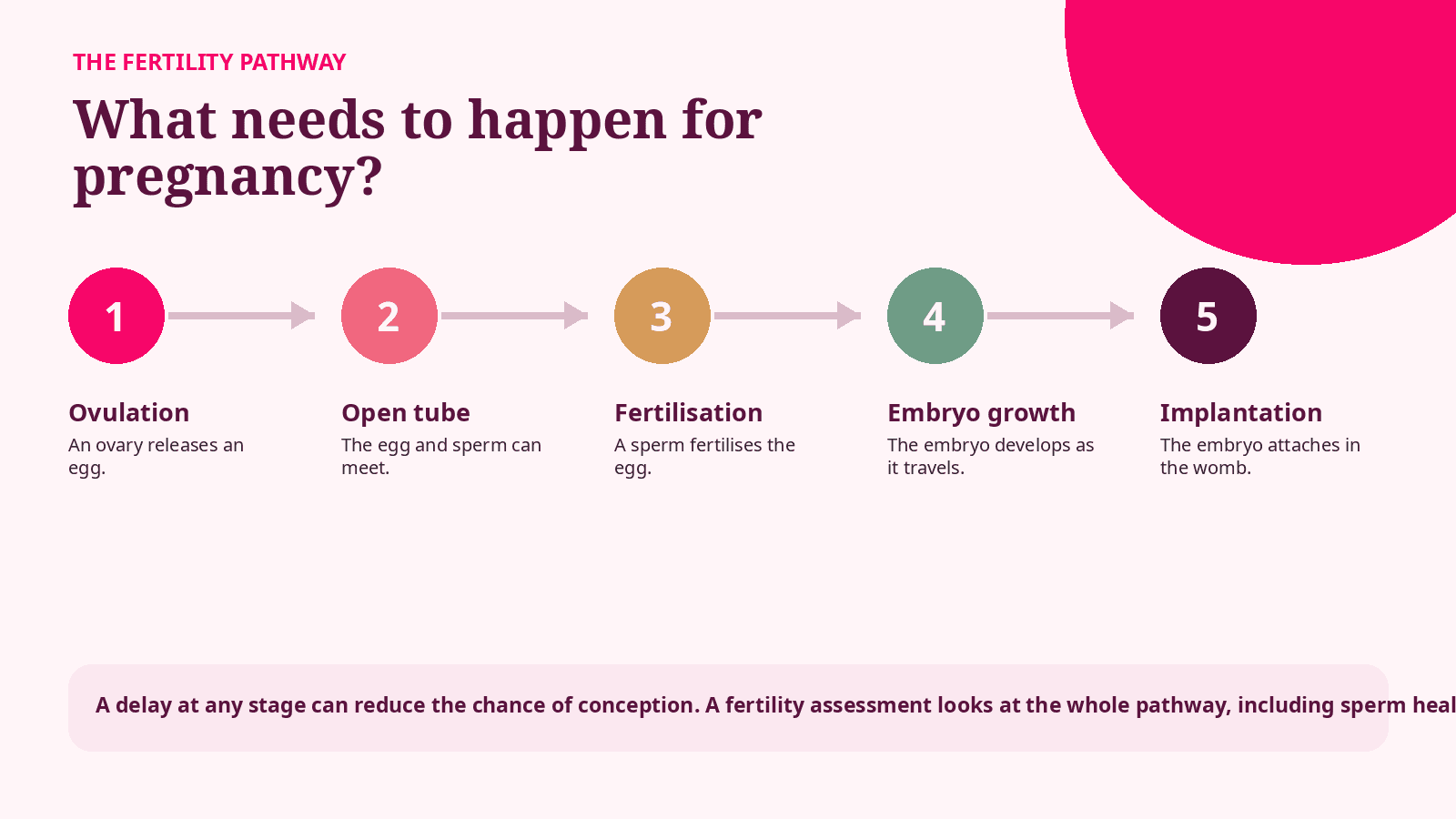
The pathway is simplified for patient education. Individual fertility journeys vary.
What can cause female infertility?
Pregnancy depends on several systems working together. A difficulty in one area may be enough to delay conception, but it is also common for more than one factor to be involved.
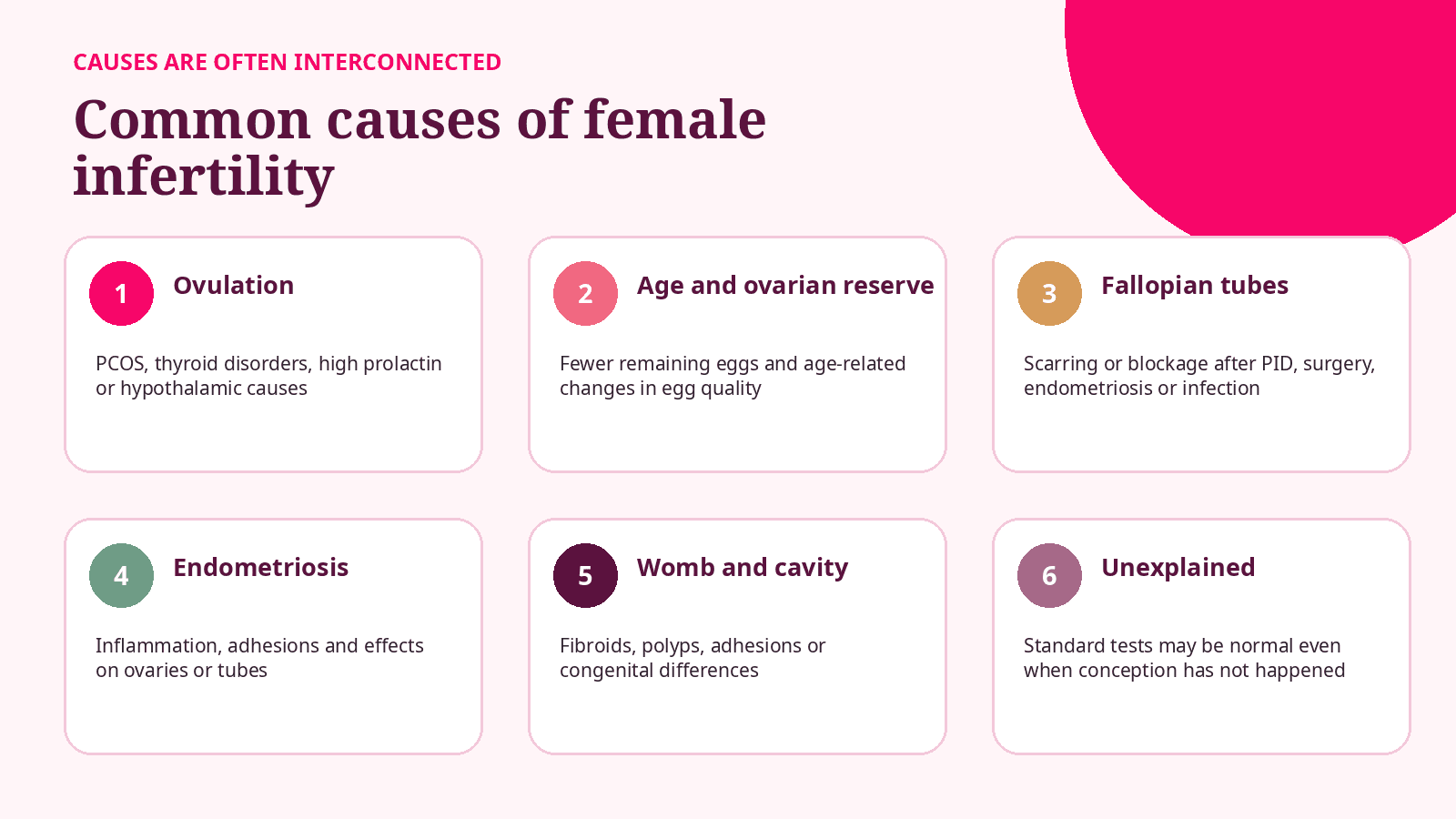
When no cause is found Unexplained infertility means that standard tests have not identified a clear reason. It does not mean the difficulty is imagined or that no biological factor exists; it means the available tests have not isolated one. |
|---|
1. Ovulation disorders
Ovulation is the release of an egg from an ovary. It may happen irregularly or not at all. Ovulation disorders are among the most common female fertility factors. [4]
Possible causes include
Polycystic ovary syndrome, or PCOS
Thyroid disorders
A high prolactin level
Hypothalamic causes linked to low weight, under-fuelling, illness or very high exercise levels
Primary ovarian insufficiency, where ovarian activity reduces before age 40
Some medicines and long-term health conditions
Possible signs
Periods that are absent, very irregular or consistently far apart
Cycles that change markedly from month to month
Symptoms linked to PCOS, thyroid disease or high prolactin
Difficulty confirming ovulation despite cycle tracking
Oocyt note Regular bleeding does not always prove that ovulation is occurring, and irregular cycles do not identify the cause on their own. Testing should be selected around your history rather than ordered as a generic package. |
|---|
2. Age, egg quality and ovarian reserve
Age is one of the strongest predictors of the chance that an egg will fertilise, develop into a chromosomally healthy embryo and result in a live birth. The decline is gradual and becomes more important through the mid-to-late thirties.
Ovarian reserve refers mainly to the remaining pool of recruitable follicles. Anti-Mullerian hormone (AMH) and antral follicle count can help estimate how the ovaries may respond to fertility medication. They do not directly measure egg quality and should not be treated as a stand-alone fertility score. [3]
AMH in plain language A lower AMH result may suggest a lower expected egg yield during stimulation. A higher result may suggest a stronger response or PCOS. Neither result can confirm whether you will conceive naturally in a particular month. |
|---|
Primary ovarian insufficiency
Primary ovarian insufficiency is reduced ovarian function before age 40. It may cause irregular or absent periods, hot flushes or fertility difficulty, although ovarian activity can be intermittent. Assessment usually includes hormones and a review of the wider medical context.
3. Fallopian tube problems
The fallopian tubes allow the egg and sperm to meet and carry the early embryo towards the womb. Scarring, blockage or fluid-filled tubes can reduce the chance of conception and may increase the risk of ectopic pregnancy.
Pelvic inflammatory disease, often linked to a previous STI
Previous ectopic pregnancy
Pelvic or abdominal surgery
Endometriosis and pelvic adhesions
Sterilisation or congenital anomalies
4. Endometriosis
Endometriosis occurs when tissue similar to the lining of the womb grows elsewhere in the pelvis. It can affect fertility through inflammation, adhesions, ovarian cysts and changes involving the tubes or ovaries. The severity of pain does not always match the extent of fertility impact.
Seek urgent medical care If you have a positive pregnancy test with one-sided lower abdominal pain, shoulder-tip pain, dizziness or unusual bleeding, seek urgent assessment because these can be symptoms of an ectopic pregnancy. |
|---|
5. The womb and uterine cavity
The womb must provide a suitable space for implantation and pregnancy. Some structural findings may affect fertility, although whether treatment improves the chance of pregnancy depends on the type, size and location of the finding.
Fibroids, particularly those that distort the uterine cavity
Endometrial polyps
Intrauterine adhesions or scar tissue
Congenital abnormalities in the shape of the womb (Uterine anomalies)
Adenomyosis, which may coexist with endometriosis
6. Cervical, sexual and medical factors
Pain during intercourse, vaginismus, erectile or ejaculatory difficulties, and cervical scarring may affect the opportunity for sperm to reach the egg. Chronic illnesses, cancer treatment and some medicines can also affect fertility. These subjects deserve sensitive, confidential discussion rather than assumptions.
Common signs of female infertility
The main sign is that pregnancy has not happened. Many people have no other symptoms. When symptoms are present, they can help guide the investigation but they do not diagnose infertility by themselves.
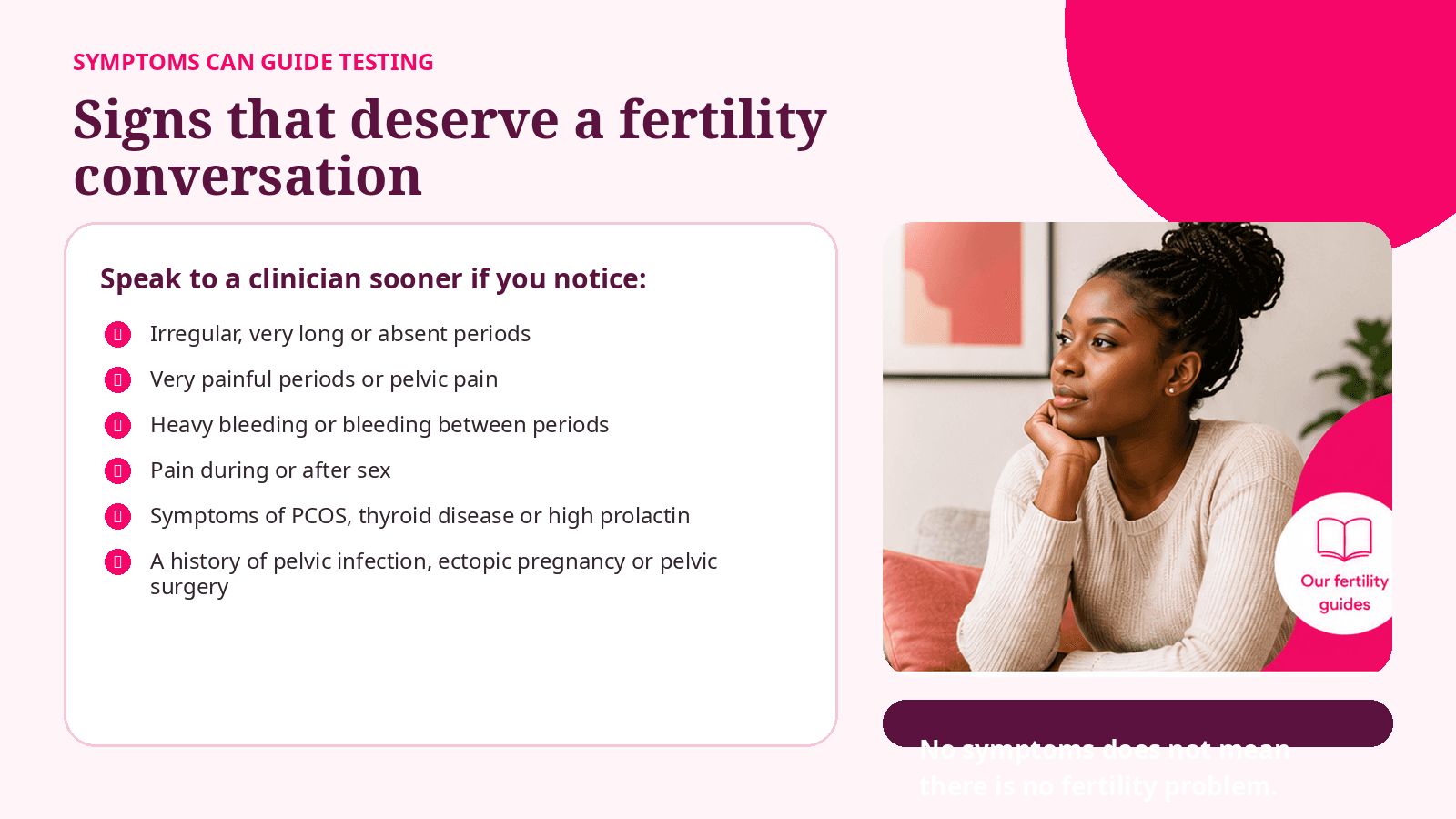
Do not wait for a symptom checklist Speak to a clinician sooner if you have a known fertility condition, previous pelvic infection or surgery, cancer treatment, very irregular or absent periods, significant pelvic pain, or concerns about either partner's fertility. |
|---|
When should you seek fertility support?
NICE recommends further assessment after 1 year of regular unprotected vaginal intercourse when pregnancy has not occurred and there is no known cause. It recommends specialist referral at presentation when the person trying to become pregnant is aged 36 or over, or when either partner has a known or suspected fertility factor. [2]
Your situation | A sensible next step |
|---|---|
Under 36, no known risk factor | Seek assessment after 12 months without pregnancy. |
Age 36 or over | Ask for specialist advice at presentation rather than waiting a year. |
Known or suspected fertility factor | Seek advice now, regardless of how long you have been trying. |
Using artificial insemination | NICE recommends assessment after 6 unsuccessful cycles when there is no known cause. |
Severe pain, absent periods or previous cancer treatment | Discuss fertility earlier because the history may change the investigation timeline. |
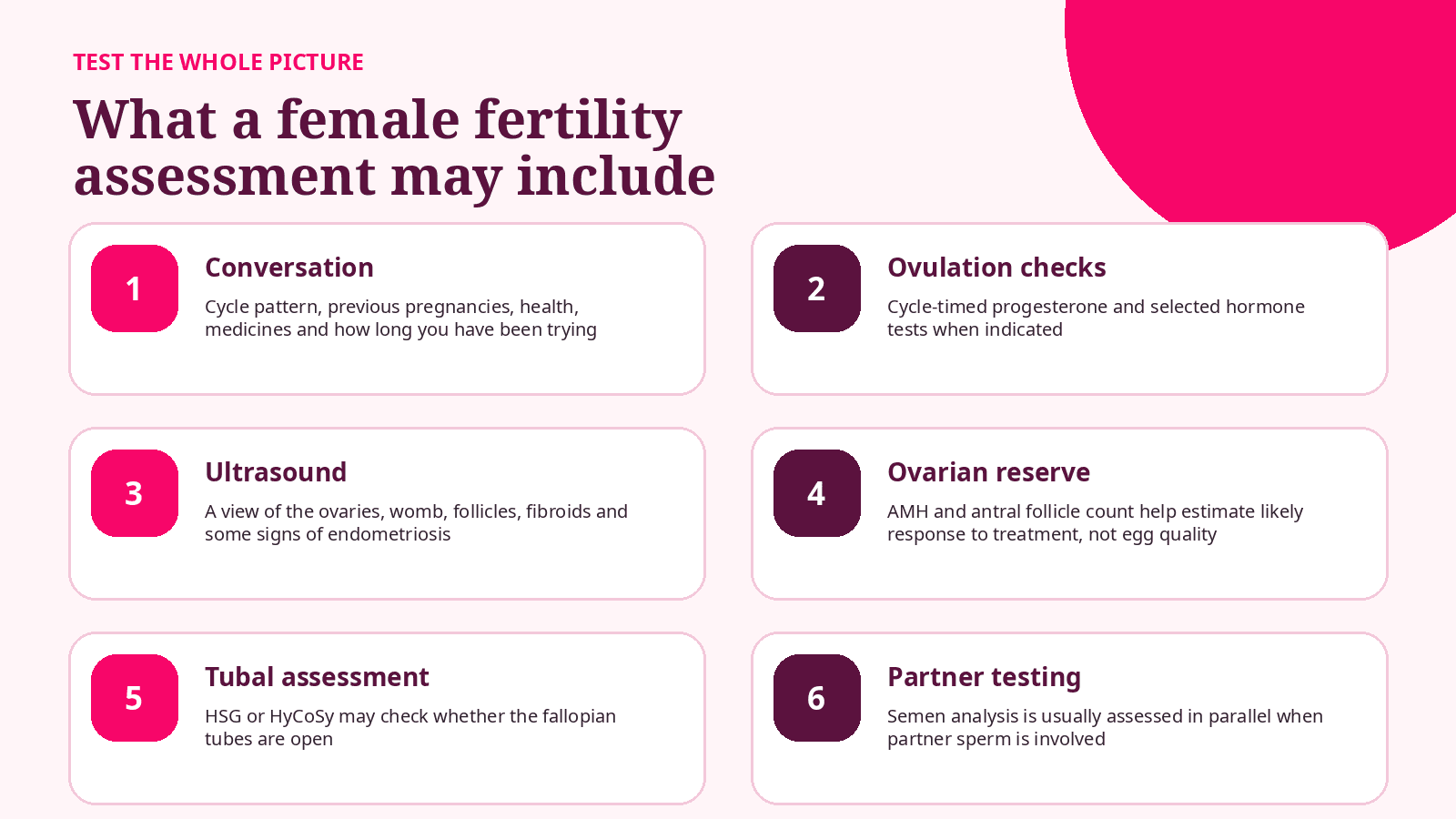
Both partners matter When a male partner is involved, semen analysis and the male fertility history should usually be considered alongside female testing. This avoids placing the whole burden of investigation on one person. |
|---|
How is female infertility assessed?
A good assessment is systematic and begins with the least invasive tests that answer the most likely questions. Testing should be personalised rather than treated as a fixed menu. [3,5]
Your clinician may also review previous pregnancy outcomes, contraception, sexual history, symptoms, medicines, family history, weight, smoking, alcohol and any previous surgery or infection. A pelvic examination is useful in selected situations but is not required for every person at the first visit.
Understanding common fertility tests
Blood tests
Progesterone can help confirm whether ovulation has occurred when timed to the individual cycle. FSH, LH, oestradiol, prolactin and thyroid tests may be useful when periods are irregular or the history suggests a hormonal cause.
AMH and antral follicle count
These estimate ovarian reserve and possible response to stimulation. They do not directly measure whether the remaining eggs are genetically healthy.
Ultrasound
A transvaginal ultrasound can assess the ovaries, follicles, womb, endometrium and findings such as fibroids or ovarian cysts. Some endometriosis is visible on specialist ultrasound, but a normal scan does not rule out all endometriosis.
Tubal patency tests
Hysterosalpingography (HSG) uses X-ray contrast, while hysterosalpingo-contrast sonography (HyCoSy) uses ultrasound contrast. The choice depends on history, local practice and whether other pelvic disease is suspected.
See https://www.oocyt.org/blog/the-complete-guide-to-fertility-blood-tests for more about testing
Tests have limits No single test can provide a complete fertility forecast. Results are most useful when interpreted together with age, cycle history, sperm results, tubal health and how long you have been trying. |
|---|
How can fertility treatment help?
Treatment depends on the cause, your age, how long you have been trying, previous pregnancies or treatment, sperm factors, funding and your own priorities. The goal is to choose an effective next step without adding unnecessary burden.
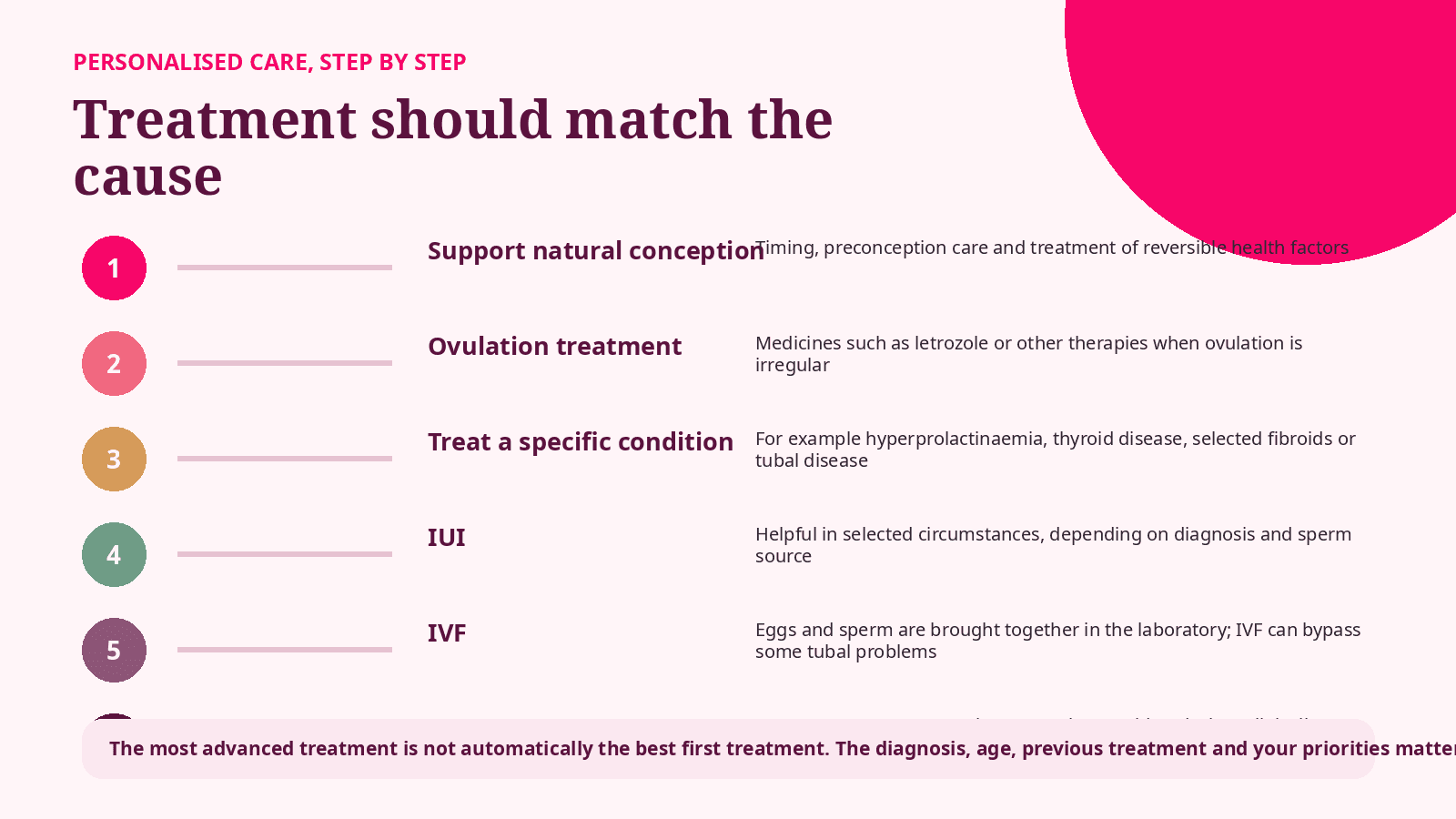
Treatment is not one-size-fits-all
Ovulation medication will not open blocked tubes. Surgery will not reverse age-related egg changes. IVF can bypass some tubal problems but does not guarantee pregnancy. A clear diagnosis helps prevent treatment from becoming a sequence of unrelated interventions.
Treatment examples by cause
Irregular ovulation or PCOS
Ovulation induction may be offered after assessment. Monitoring and the exact medicine depend on the diagnosis and clinical pathway. See our series on Ovulation induction for more https://www.oocyt.org/blog/letrozole-success-rates
High prolactin
Treating the underlying cause and using medicines such as cabergoline may restore ovulation in appropriate patients. NICE recommends cabergoline for ovulatory disorders caused by hyperprolactinaemia. [2]
Mild tubal disease
Selected people may be offered tubal surgery where expertise is available. IVF may be more appropriate when disease is severe or other factors are present.
Endometriosis
Options may include expectant management, surgery, IUI in selected cases or IVF. Age, symptoms, ovarian reserve, male factors and treatment preferences should shape the discussion. [2]
Fibroids, polyps or adhesions
Treatment is considered when the position or extent is likely to affect the cavity, tubes, implantation or symptoms. Not every fibroid needs removal.
Reduced ovarian reserve or older reproductive age
The conversation may become more time-sensitive. IVF, fertility preservation or donor eggs may be discussed depending on the situation.
Can lifestyle changes improve fertility?
Lifestyle is part of fertility health, but it should not be used to blame people for infertility. Many fertility conditions are not caused by lifestyle and cannot be corrected by willpower.
Stop smoking and avoid exposure to tobacco smoke
Discuss alcohol intake while trying to conceive
Aim for sustainable nutrition and movement rather than crash dieting
Take preconception folic acid as advised for your circumstances
Review prescription medicines, supplements and long-term conditions with a clinician
Protect yourself from STIs and seek treatment promptly when needed
A balanced message Healthy changes can support fertility and pregnancy health, but they cannot unblock a fallopian tube, remove endometriosis or reverse reproductive ageing. They should sit alongside appropriate investigation and treatment. |
|---|
The emotional side of female infertility
Trying to conceive can affect mood, confidence, intimacy, work, friendships and relationships. Women may also face unfair blame or stigma even when male factors or combined factors are involved. Your emotional response is valid, and support should be part of fertility care rather than an afterthought. [1]
 | Support can include
|
|---|---|
You are allowed to pause Taking time to process information or seek a second opinion is not giving up. Urgency may matter in some circumstances, but informed consent still requires space to understand your options. |
|---|
Frequently asked questions
Can I have regular periods and still have infertility?
Yes. Regular cycles are reassuring but do not confirm tubal patency, egg quality, sperm health, endometriosis or implantation.
Does a low AMH result mean I cannot get pregnant?
No. AMH mainly estimates ovarian reserve and treatment response. Age and the wider fertility picture are essential to interpretation.
Can fibroids cause infertility?
Some can, particularly if they distort the uterine cavity or block a tube. Many fibroids do not affect fertility, so location matters more than the word fibroid alone.
Is IVF always the next step?
No. The right next step may be further testing, ovulation treatment, surgery, IUI, IVF or continued attempts, depending on the cause and circumstances.
What if all my tests are normal?
You may be given a diagnosis of unexplained infertility. Your clinician should still discuss prognosis and evidence-based options rather than imply that nothing is wrong.
Should my partner be tested too?
When partner sperm is involved, yes. Fertility problems may involve either or both partners, and parallel assessment can prevent unnecessary delay.
The bottom line
Female infertility is a starting point for investigation - not a conclusion about your future. Understanding ovulation, age, ovarian reserve, the fallopian tubes, endometriosis, the womb and sperm factors allows care to become more specific. The right plan is the one that fits the evidence and the person. |
|---|
Ask your clinician what each test is intended to answer, how the result would change the plan, and when your treatment should be reviewed. Clear questions can protect you from unnecessary tests, delays and add-ons.
Considering fertility treatment? Start with clarity.
Oocyt helps you understand your options, compare fertility pathways and prepare for informed conversations with clinics locally or internationally.
References
1. World Health Organization (2025). Infertility: fact sheet and Guideline for the prevention, diagnosis and treatment of infertility.
2. National Institute for Health and Care Excellence (2026). Fertility problems: assessment and treatment. NICE guideline NG257.
3. American Society for Reproductive Medicine (2021). Fertility evaluation of infertile women: a committee opinion. Fertility and Sterility, 116(5), 1255-1265.
4. NHS (accessed July 2026). Causes of infertility.
5. NHS (accessed July 2026). Diagnosis of infertility.
6. National Institute for Health and Care Excellence. Endometriosis: diagnosis and management. NICE guideline NG73.
7. International Evidence-Based Guideline for the Assessment and Management of Polycystic Ovary Syndrome (2023).
Editorial disclaimer Oocyt provides fertility education, navigation and support services. We do not diagnose, prescribe or replace personalised medical care. Medical decisions should be made with qualified healthcare professionals and your treating clinic. |
|---|