Fertility Basics
Amatoritsero Olumami-Oyibo ·
18 min read


FERTILITY EDUCATION
Medical information, not personal medical advice Male fertility problems can have hormonal, genetic, anatomical, medical and lifestyle causes. This guide cannot diagnose an individual result. A qualified fertility or male reproductive specialist should interpret semen tests and recommend treatment in the context of both partners and your family-building goals. |
The first test is usually a semen analysis, but a result is not a verdict. Sperm measurements vary between samples, and a number outside a reference range does not automatically mean natural conception is impossible. The purpose of assessment is to identify the cause, look for wider health implications and decide whether treatment, assisted conception or continued trying is appropriate.
Oocyt clinical insight Male fertility assessment should begin alongside the assessment of the person providing eggs or carrying the pregnancy. It should not be treated as an afterthought after months of tests or unsuccessful treatment. |
What this guide covers
What male factor infertility means and why the terms mild, moderate and severe can be misleading.
How semen analysis works and why an abnormal result may need to be repeated.
Common causes of low sperm count, reduced motility, abnormal morphology and ejaculation problems.
What azoospermia means, including obstructive and non-obstructive azoospermia.
How male infertility is investigated, including hormone, genetic and imaging tests.
Treatment options, including targeted medical treatment, surgery, IUI, IVF, ICSI and surgical sperm retrieval.
What a varicocele is and when treatment may be considered.
Warning signs, lifestyle considerations, emotional support and questions to ask your clinician.

At a glance
Main first test | Semen analysis. |
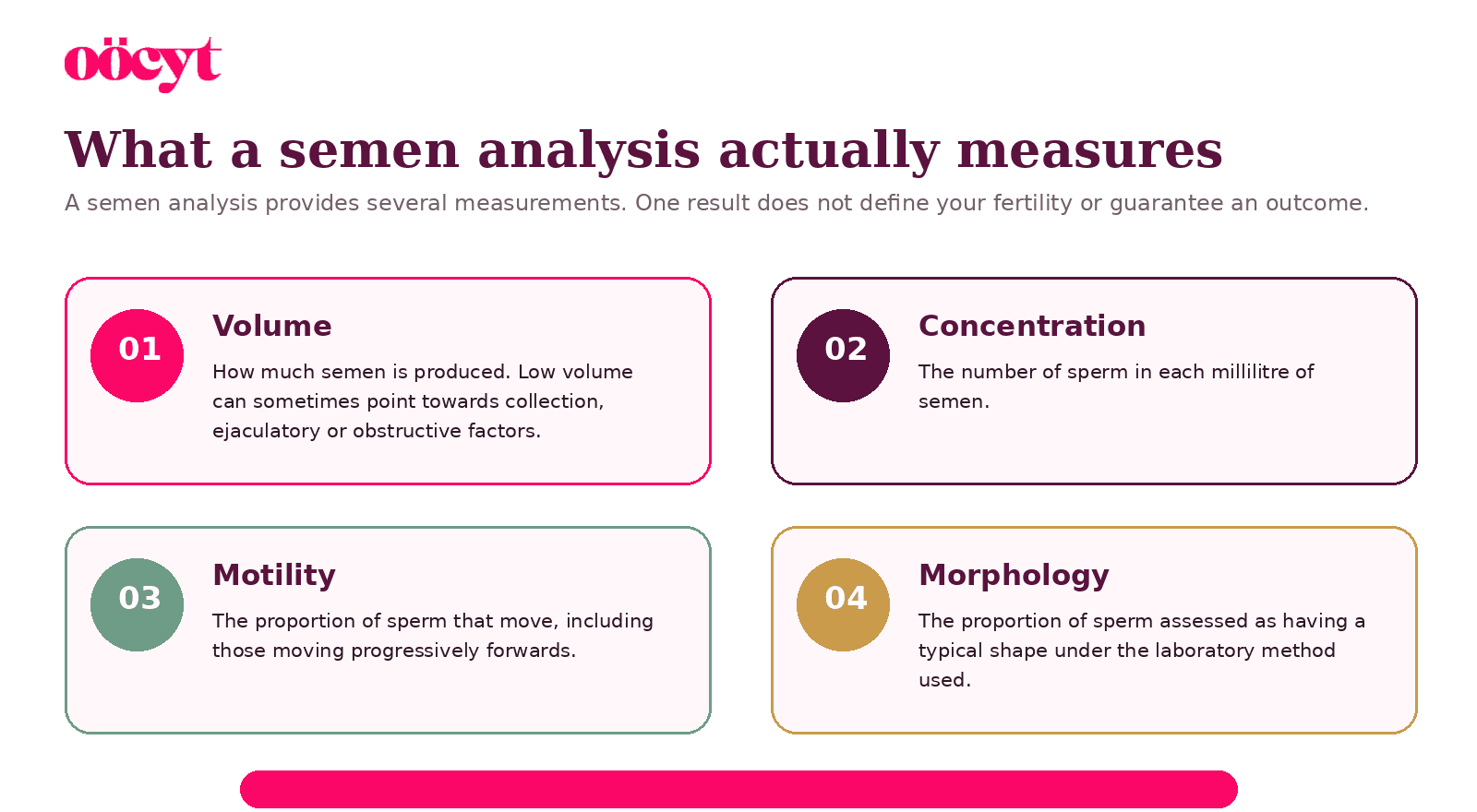
What it measures | Semen volume, sperm concentration, motility and morphology. |
If abnormal | Repeat testing and specialist assessment may be needed. |
Azoospermia | No sperm found in the ejaculate after appropriate laboratory examination. |
Common treatments | Cause-specific treatment, IUI, IVF, ICSI, surgery or sperm retrieval. |
Important warning | Testosterone and anabolic steroids can suppress sperm production. |
What is male factor infertility?
Male factor infertility describes a situation in which a factor related to sperm, ejaculation, sexual function or the male reproductive system reduces the chance of conception. It may be the only identified cause, one of several contributing factors, or part of a fertility problem that remains unexplained after standard testing. [1,3]
A male fertility problem is not a judgment about masculinity, sexual ability or worth. Many men with abnormal sperm results have no symptoms, and many men with normal sexual function can still have a sperm-related fertility problem.
Why “mild, moderate and severe” is not a complete diagnosis
The source material divided male factor infertility into three fixed levels. In practice, there is no universal three-stage classification that accurately predicts pregnancy or determines treatment. A result may look mildly abnormal but matter more when time is limited, while a severe result may have a treatable cause or still allow sperm retrieval and ICSI.
Clinicians interpret the complete picture: several semen parameters, whether abnormalities are repeated, the cause, previous pregnancies, sexual function, age and fertility factors affecting the partner, and the length of time trying.
A better question Instead of asking “How severe is my male factor?”, ask: “What is causing the result, can anything be treated, and which route gives us a realistic chance of pregnancy?” |
Male factors should be assessed early
Current male infertility guidance recommends parallel evaluation of both partners because focusing only on the person carrying the pregnancy can delay diagnosis and expose them to unnecessary tests or treatment. Some causes of abnormal sperm production can also be linked to wider health conditions, so specialist review is valuable beyond fertility alone. [2,3]
Understanding semen analysis
A semen analysis examines a fresh semen sample in a specialist laboratory. It is usually the starting point for male fertility assessment because it provides information about sperm number and function as well as the semen carrying the sperm. [2,5]
A reference range is not a pass-or-fail line
WHO reference values describe the distribution of results in men whose partners conceived within a defined period. They do not separate fertile from infertile people with certainty. Pregnancy can occur with results below a reference limit, and a normal result cannot guarantee conception. [5]
Why a semen analysis may be repeated
Sperm production changes over time. Fever, illness, collection difficulties, abstinence interval, medicines and laboratory variation can all affect a sample. NICE recommends a repeat confirmatory test when the first semen analysis is abnormal, ideally after around three months, although azoospermia or severe oligozoospermia should be repeated sooner. [2]
Before providing a sample Follow the laboratory’s instructions carefully, including the requested abstinence interval, how to collect the full sample and how quickly it must reach the laboratory. Tell the clinic if any of the sample was lost. |
What can cause male factor infertility?
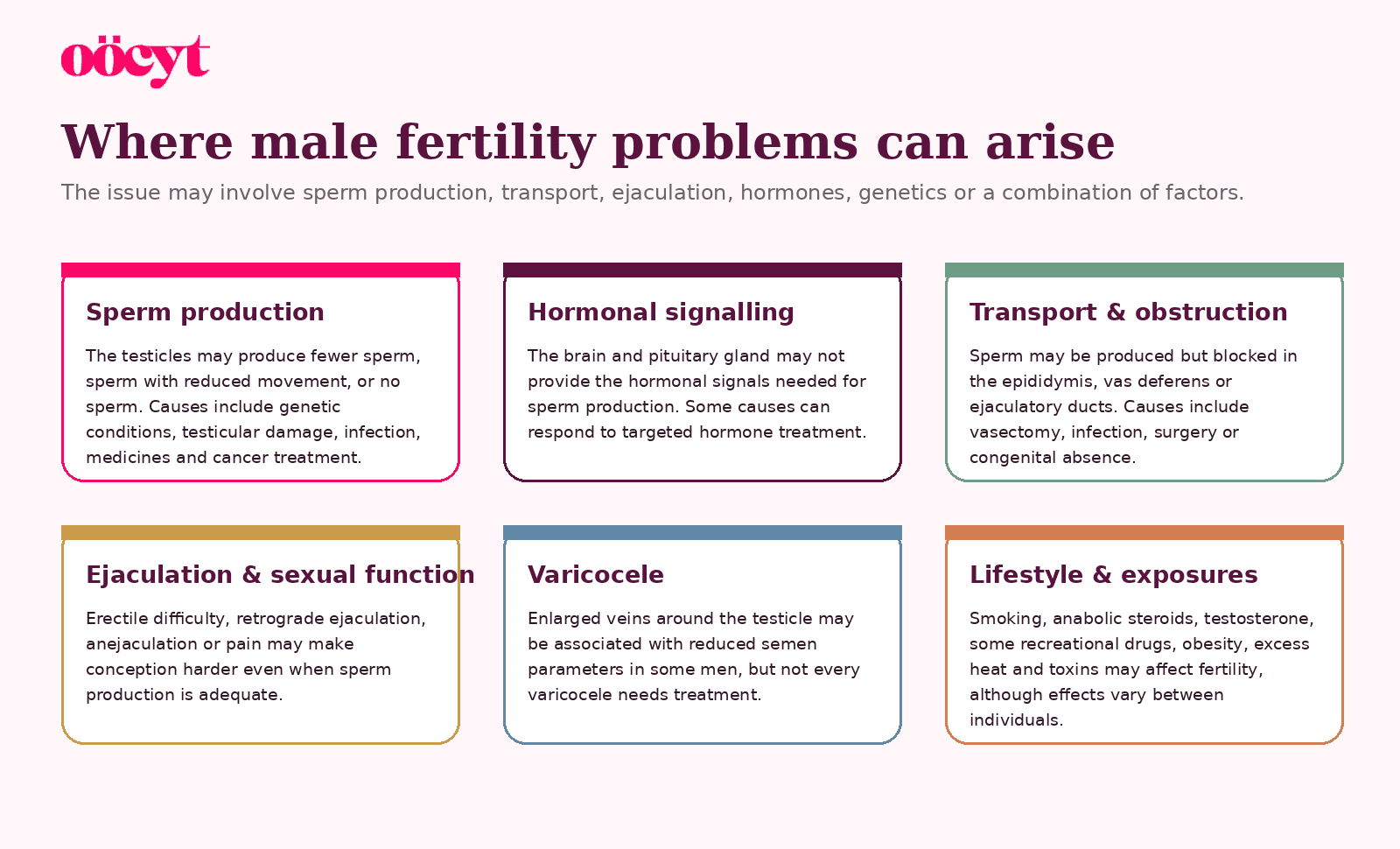
Male fertility depends on hormonal signalling, healthy testicular tissue, sperm production, unobstructed transport and successful ejaculation. A problem can arise at any point, and more than one factor may be present.
Common medical and reproductive causes
Genetic conditions, including Klinefelter syndrome, Y-chromosome microdeletions and CFTR-related absence or blockage of the vas deferens.
Undescended testes, testicular torsion, injury, orchitis or previous testicular surgery.
Hormonal conditions affecting the hypothalamus, pituitary gland or testicles.
Chemotherapy, radiotherapy and some medicines or toxins.
Infection, inflammation, scarring, vasectomy or another obstruction in the reproductive tract.
Erectile dysfunction, ejaculatory failure, retrograde ejaculation or anejaculation.
Varicocele in selected men with reduced semen parameters.
No identifiable cause despite appropriate assessment.
How sperm are produced and delivered
Sperm are produced inside the testicles, mature in the epididymis and travel through the vas deferens. During ejaculation, sperm mix with fluids from the seminal vesicles and prostate before leaving through the urethra.

Production problems versus delivery problems
This distinction is central to azoospermia. If sperm production is relatively preserved but there is a blockage, the condition is obstructive azoospermia. If the testicle is producing very few or no sperm, the condition is non-obstructive azoospermia. Hormonal failure can also reduce the signal needed for sperm production and may be grouped with non-obstructive causes.
|
What is azoospermia?
Azoospermia means that no sperm are found in the ejaculate after appropriate laboratory examination. It is identified in roughly 10% of infertile men. The diagnosis should be confirmed, because a single sample may be affected by collection problems or very rare sperm that are only found after careful centrifugation and examination. [2,9]
Azoospermia does not always mean that the testicles produce no sperm. Sperm may be produced but prevented from reaching the ejaculate, or production may occur only in small isolated areas of testicular tissue.

What is cryptozoospermia?
Cryptozoospermia means that sperm are not seen in the initial examination but a very small number are found after the sample is concentrated and searched carefully. This is different from confirmed azoospermia and may affect the plan for sperm freezing, IVF timing and surgical retrieval.
Obstructive azoospermia
In obstructive azoospermia, sperm production is usually present, but sperm cannot reach the ejaculate. A blockage may be congenital or acquired.
Possible causes
Vasectomy or a previous unsuccessful vasectomy reversal.
Scarring after infection, inflammation, injury or pelvic surgery.
Congenital bilateral absence of the vas deferens, which may be associated with CFTR gene variants.
Blockage in the epididymis or ejaculatory ducts.
Ejaculatory disorders that prevent sperm-containing semen from leaving normally.
How it may be investigated
Clues can come from semen volume, hormone levels, testicular size and examination of the vas deferens. Genetic testing, ultrasound or urine testing may be recommended depending on the suspected site and cause of obstruction. [3,8]
Treatment options
NICE recommends offering either surgical correction or surgical sperm retrieval for obstructive azoospermia. The decision should take account of the duration and site of obstruction, risks and benefits, personal preference and fertility factors affecting the partner, including age, ovarian reserve, ovulation and tubal health. [2]
Microsurgical reconstruction or vasectomy reversal when appropriate.
Retrieval of sperm from the epididymis or testicle for use with ICSI.
Treatment of an ejaculatory disorder using the least invasive effective approach.
A diagnosis still matters when IVF is planned ICSI may bypass an obstruction, but understanding the cause can identify genetic implications, offer the possibility of reconstruction and help the couple choose between surgery and assisted conception. |
Non-obstructive azoospermia
In non-obstructive azoospermia, sperm production within the testicle is severely impaired. The degree and pattern of impairment vary. Some men have no retrievable sperm, while others have small areas of active sperm production that can be identified surgically.
Possible causes
Klinefelter syndrome or another chromosome condition.
Y-chromosome microdeletions.
Previous undescended testes, torsion, injury, infection or testicular cancer treatment.
Chemotherapy, radiotherapy or gonadotoxic medicines.
Severe hormonal signalling disorders.
Anabolic steroid or testosterone use that has suppressed natural sperm production.
No identifiable explanation after testing.
Hormone and genetic assessment
Hormone tests can help distinguish impaired testicular production from inadequate stimulation by the brain or pituitary gland. Men with azoospermia or severe oligozoospermia may be offered a karyotype and Y-chromosome microdeletion testing, depending on the clinical picture. Genetic counselling may be important before ICSI because some genetic causes can be passed to children. [3,8]
Important genetic exception Current NICE guidance says surgical sperm retrieval should not be offered when a complete Y-chromosome AZFa or AZFb microdeletion is present, because successful retrieval is not expected. [2] |
Can sperm be retrieved?
NICE recommends offering surgical sperm retrieval for non-obstructive azoospermia and considering microdissection testicular sperm extraction, known as micro-TESE. Retrieval is not guaranteed. Success depends strongly on the underlying cause, genetic findings, previous treatment and testicular pathology. [2,7,9]
How male factor infertility is diagnosed
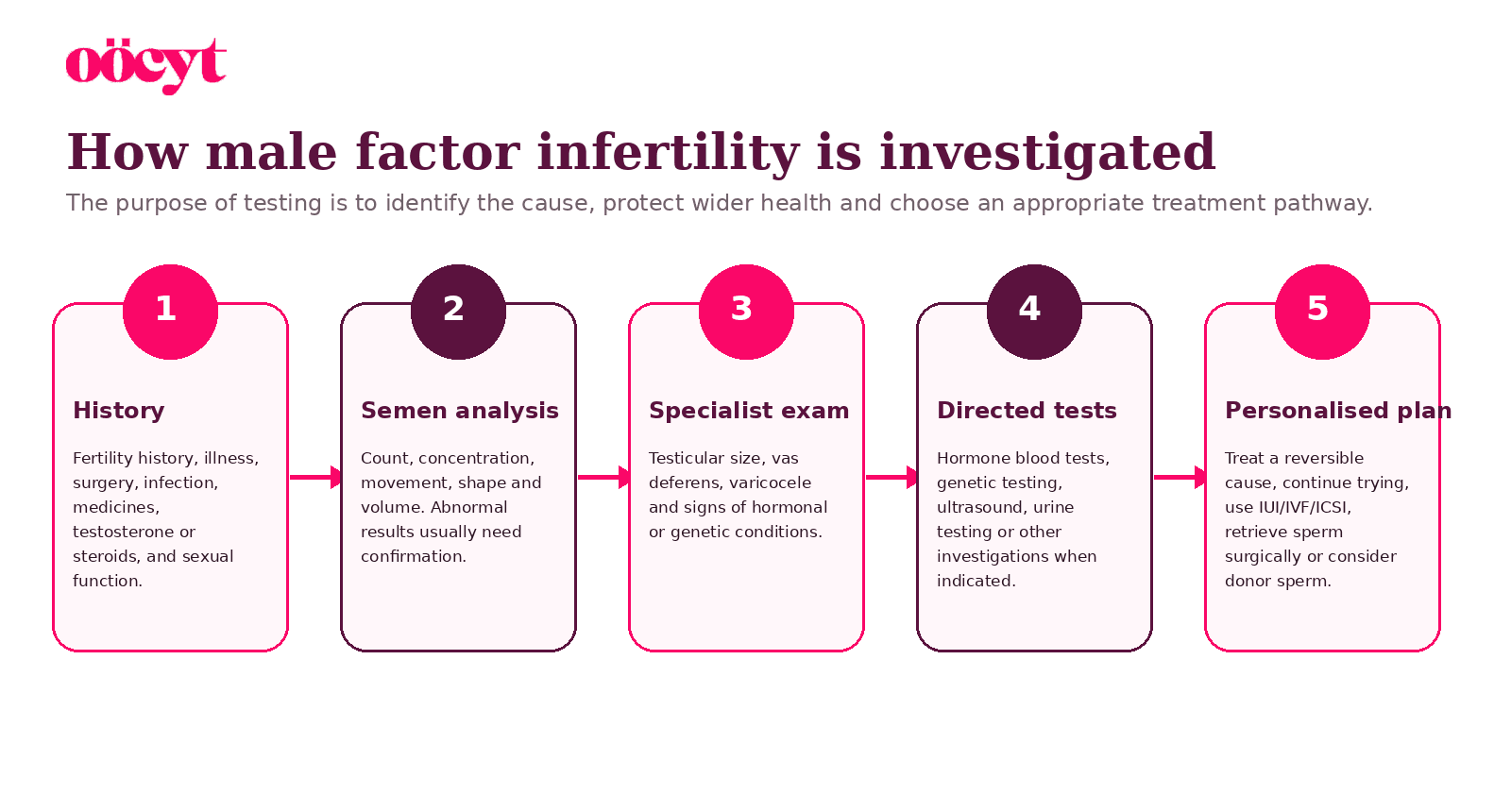
A careful assessment goes beyond ordering one sperm test. It combines semen results with medical history, examination and targeted investigations.
Your clinician may ask about
Previous pregnancies, duration of trying and timing of intercourse or insemination.
Childhood undescended testes, mumps orchitis, torsion, testicular trauma or surgery.
Pelvic surgery, hernia repair, infection, vasectomy or urinary symptoms.
Chemotherapy, radiotherapy, medicines, testosterone, anabolic steroids and supplements.
Erections, ejaculation, libido and pain during sex or ejaculation.
Smoking, alcohol, recreational drugs, occupation, heat and chemical exposures.
Family history of infertility, cystic fibrosis, congenital differences or genetic conditions.
Possible tests after semen analysis
Hormone blood tests such as FSH, LH, testosterone and prolactin when indicated.
Karyotype, Y-chromosome microdeletion or CFTR testing in selected cases.
Scrotal or transrectal ultrasound when examination or semen findings suggest a structural problem.
Post-ejaculatory urine testing if retrograde ejaculation is suspected.
Further specialist laboratory testing only when it is likely to change management.
Treatment should match the cause
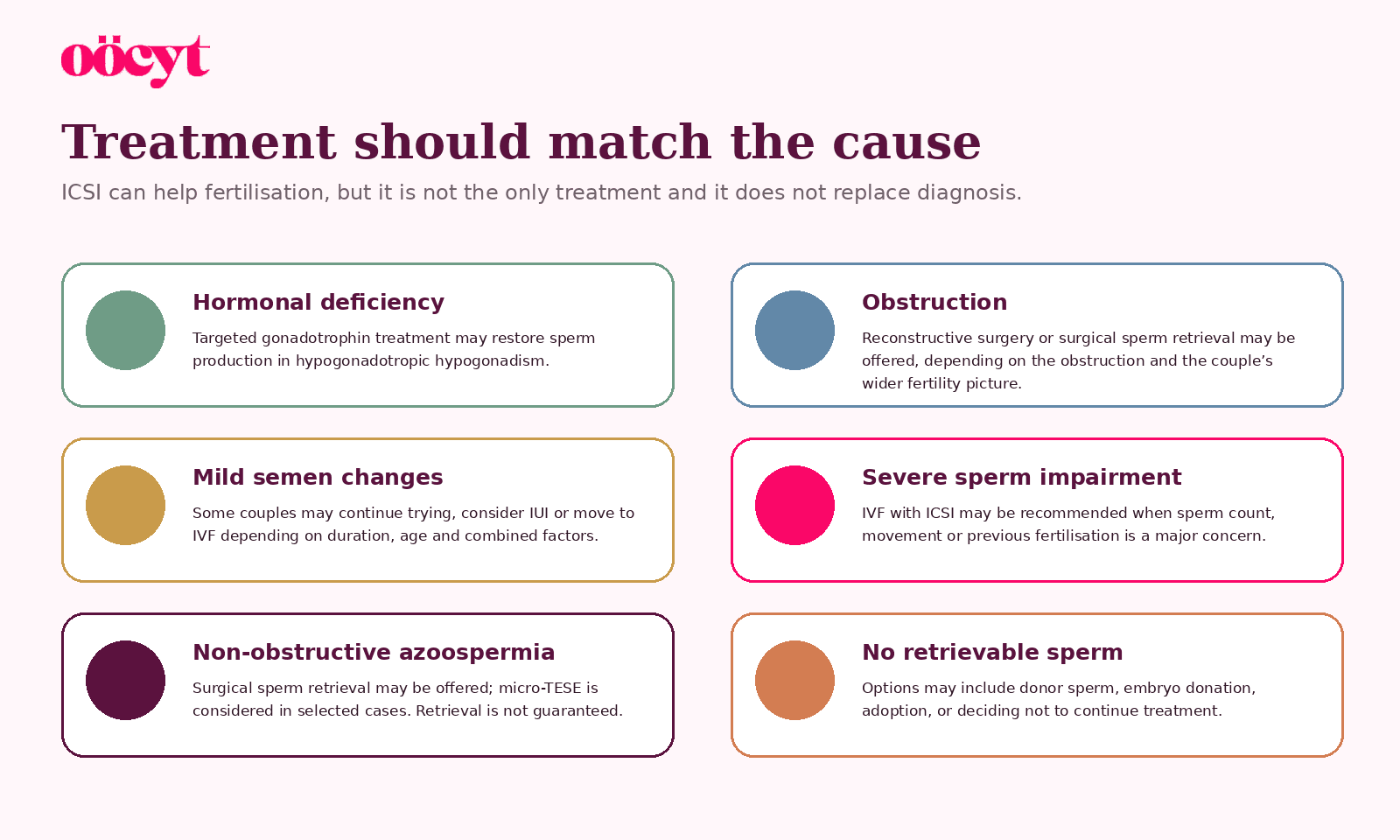
There is no single treatment for male factor infertility. Some causes can be corrected, some can be bypassed with assisted conception, and some require a discussion about donor sperm or other family-building routes.
Medical treatment
Targeted gonadotrophin treatment can stimulate sperm production in hypogonadotropic hypogonadism. Current NICE guidance does not recommend androgens such as testosterone to treat semen abnormalities, and hormone or anti-oestrogen therapy for other impaired semen parameters should only be considered within a clinical trial. [2]
Supplements and antioxidants
Many products are marketed as sperm boosters. Evidence is inconsistent, doses vary and supplements can interact with medicines. NICE advises against offering supplements, antioxidants or medical treatments specifically to improve sperm DNA integrity. Do not let supplements delay diagnosis of a treatable cause. [2]
IUI, IVF and ICSI
Intrauterine insemination (IUI)
Prepared sperm are placed into the uterus around ovulation. IUI may be considered when sperm numbers and movement are adequate after preparation and there are no major female fertility barriers. It is not generally suitable for severe sperm impairment or azoospermia.
In vitro fertilisation (IVF)
Eggs are collected and mixed with sperm in a laboratory. Conventional IVF relies on sperm reaching and fertilising the egg without direct injection.
Intracytoplasmic sperm injection (ICSI)
In ICSI, an embryologist injects one sperm directly into an egg. It is commonly used for severe sperm abnormalities, surgically retrieved sperm or previous poor fertilisation. ICSI can overcome some barriers to fertilisation, but it does not correct the underlying cause or guarantee embryo development, implantation or live birth. [4,6]
ICSI is not a substitute for male assessment A diagnosis can reveal a reversible condition, a genetic issue, a health concern or a sperm-retrieval option. The male partner should not disappear from the pathway once ICSI is mentioned. |
Surgical sperm retrieval
Sperm may be collected from the epididymis or testicle using techniques such as PESA, MESA, TESA, TESE or micro-TESE. The appropriate procedure depends on whether the problem is obstructive or non-obstructive, local expertise and the planned fertility treatment. Surgically retrieved sperm are usually used with ICSI. [2,7,9]
Clinics may retrieve and freeze sperm before ovarian stimulation, or coordinate retrieval with egg collection in selected cases. Coordinating procedures can avoid unnecessary treatment, but it also creates the risk that no sperm are found on the day. This decision needs careful counselling and a contingency plan.
Varicocele and fertility
A varicocele is an enlargement of veins around a testicle, most often on the left side. It may feel like a soft bag of worms when standing, but many varicoceles cause no symptoms and are found during examination.
Possible symptoms
A dull ache or dragging discomfort, often worse after standing or exertion.
Visible or palpable enlarged veins in the scrotum.
A smaller or softer affected testicle.
Reduced semen parameters discovered during fertility testing.
Does every varicocele need treatment?
No. Many varicoceles do not affect fertility, and treating a varicocele found only on ultrasound is not automatically beneficial. NICE says to consider radiological or surgical treatment when the varicocele is detected on clinical examination, semen parameters are reduced and the couple is trying to conceive spontaneously, while taking female fertility factors into account. [2]
Seek urgent advice for sudden testicular pain Sudden severe testicular pain is not typical of a varicocele and needs urgent medical assessment to exclude testicular torsion or another acute condition. |
Warning signs and when to seek help
Male factor infertility often causes no symptoms. Semen analysis may be the only way to identify a problem. However, certain symptoms and medical histories justify earlier assessment.
Speak to a clinician sooner if you have
A testicular lump, persistent swelling, pain or a noticeable difference in testicular size.
Difficulty getting or maintaining an erection, very low libido or pain with ejaculation.
Dry orgasm, very low semen volume, cloudy urine after orgasm or inability to ejaculate.
A history of undescended testes, torsion, testicular cancer, pelvic surgery or vasectomy.
Previous chemotherapy, radiotherapy or a medicine known to affect fertility.
Current or previous testosterone or anabolic steroid use.
A known genetic condition or family history of infertility or cystic fibrosis.
Do not wait if you feel a lump A new testicular lump should be assessed promptly. Most lumps are not cancer, but a clinician needs to examine them and arrange ultrasound when appropriate. |
Lifestyle, medicines and sperm health
Lifestyle changes cannot overcome every fertility diagnosis, and patients should not be blamed for medical or genetic causes. However, reducing avoidable exposures can support general health and may improve semen parameters for some people over the months required to produce new sperm.
The testosterone warning
Testosterone replacement and anabolic steroids can suppress the hormonal signals that drive sperm production. They may cause very low sperm counts or azoospermia. Never start testosterone for fertility, and do not stop prescribed treatment abruptly without speaking to the clinician managing it. Tell your fertility specialist about injections, gels, bodybuilding drugs and over-the-counter performance products. [2,10]
Practical steps
Stop smoking and avoid recreational drugs.
Keep alcohol within recommended limits and discuss whether reducing further is appropriate while trying to conceive.
Aim for a sustainable weight, regular movement and a balanced diet.
Avoid prolonged or extreme heat exposure to the testicles where practical.
Use protective equipment at work and follow guidance around pesticides, solvents, heavy metals and radiation.
Review medicines with a clinician rather than stopping them yourself.
Have regular intercourse every 2 to 3 days when trying naturally; very long abstinence is not necessary.
Sperm changes take time Sperm production takes around three months. A lifestyle or medical change will not usually be reflected immediately in a semen analysis. |
The emotional impact of male infertility
A sperm-related diagnosis can affect confidence, identity, sex and relationships.
|  |
You are more than a result
Low sperm count, azoospermia or a failed retrieval does not define your masculinity or your value as a partner. It is reasonable to grieve, seek a second opinion, pause treatment or change the family-building plan.
Oocyt support Oocyt can help you understand terminology, prepare questions, compare clinics and navigate treatment locally or internationally. Medical diagnosis and treatment remain with qualified clinicians, but you do not have to work out the pathway alone. |
Questions to ask at your appointment
Does this result need to be repeated, and how soon?
Which findings suggest reduced production, obstruction or an ejaculation problem?
Do I need hormone, genetic or imaging tests?
Is there a reversible cause or a medicine that may be suppressing sperm production?
What is the realistic chance of natural conception, IUI, IVF or ICSI in our complete situation?
Should sperm be frozen before treatment or surgery?
What happens if no sperm are retrieved?
Frequently asked questions
Can an abnormal semen analysis improve?
Yes, depending on the cause. Results may recover after fever, stopping suppressive drugs under medical supervision, treating hormonal deficiency or correcting selected conditions. Other causes are permanent or only partly reversible.
Does azoospermia mean I cannot have a biological child?
No. Some obstructive causes can be reconstructed, and sperm can often be retrieved when production is present. In non-obstructive azoospermia, micro-TESE may find sperm in selected men, but retrieval is not guaranteed.
Is IVF the only option for azoospermia?
It depends on the cause. Obstructive azoospermia may be treated by reconstruction or by sperm retrieval with ICSI. Hormonal azoospermia may respond to treatment. When sperm must be surgically retrieved, ICSI is generally required to use them.
Can ICSI fix poor sperm quality?
ICSI helps a sperm enter an egg. It does not repair sperm DNA, treat the cause, ensure normal embryo development or guarantee pregnancy.
Should I take testosterone if my testosterone is low?
Not while trying to conceive unless managed in a specialist fertility pathway. External testosterone can shut down the signals needed for sperm production and may cause azoospermia.
Do supplements improve sperm DNA fragmentation?
Evidence is uncertain. NICE advises against offering supplements, antioxidants or medical treatment specifically to improve sperm DNA integrity. Discuss products with a clinician.
Can a varicocele cause infertility?
It can be associated with reduced semen parameters in some men. Many varicoceles cause no fertility problem. Treatment is considered selectively, not automatically.
Can male age affect fertility?
Male fertility usually declines more gradually than female fertility, but sperm quality and some risks can change with age. The effect should be considered alongside the age and health of the person providing eggs.
When should we get help?
Usually after 12 months of regular unprotected intercourse, earlier when the partner providing eggs is 36 or over, and promptly when there is a known male fertility risk, symptom or abnormal result.
The bottom line
A male fertility diagnosis should create clarity, not blame Male factors contribute to around half of infertility cases. A semen analysis is the beginning of an investigation, not the end of the story. The right pathway identifies whether the issue involves production, transport, hormones, ejaculation or a combination, then matches treatment to the cause and the couple’s complete fertility picture. |
Your next steps
Arrange or repeat a semen analysis through an accredited laboratory.
Ask for specialist male reproductive assessment when abnormalities are confirmed or azoospermia is suspected.
Review medicines, testosterone, anabolic steroids and relevant medical history honestly with the clinician.
Complete both partners’ fertility assessment in parallel.
Ask for a written plan covering natural conception, treatment options, review points and contingencies.
Ready for clearer fertility guidance?
Oocyt helps you understand fertility options, compare clinics and prepare for the next step with realistic information and compassionate support.
References
1. World Health Organization (2025). Infertility: fact sheet. View source
2. NICE (2026). Fertility problems: assessment and treatment. NICE guideline NG257. View source
3. American Urological Association and American Society for Reproductive Medicine (2020/2021). Diagnosis and treatment of infertility in men: guideline, Part I. View source
4. American Urological Association and American Society for Reproductive Medicine (2020/2021). Diagnosis and treatment of infertility in men: guideline, Part II. View source
5. World Health Organization (2021). WHO laboratory manual for the examination and processing of human semen, 6th edition. View source
6. Human Fertilisation and Embryology Authority. Intracytoplasmic sperm injection (ICSI). View source
7. Human Fertilisation and Embryology Authority. Surgical sperm extraction. View source
8. European Association of Urology. Sexual and Reproductive Health Guidelines: Male Infertility. View source
9. NICE (2026). Evidence review for surgical sperm retrieval techniques. View source
10. Leeds Teaching Hospitals NHS Trust (2026). Fertility services and treatments: male lifestyle and testosterone advice. View source
Editorial disclaimer Oocyt provides fertility education, guidance and support services only. We do not provide medical advice, diagnosis or treatment. Medical decisions should be made with licensed healthcare professionals and your treating clinic. |