Treatment Journeys
Amatoritsero Olumami-Oyibo ·
12 min read

FERTILITY EDUCATION
Medical information, not personal medical advice This guide provides general fertility education. Your age, cycle pattern, metabolic health, partner or donor sperm results, tubal health and personal goals affect which options may be appropriate. Speak to a qualified fertility clinician about your individual circumstances. |
|---|
In this guide
What PCOS - now also called PMOS - means
How PCOS affects ovulation and fertility
How to improve your preconception health without chasing a “perfect” lifestyle
Which fertility tests matter before treatment
Letrozole, metformin, clomiphene, gonadotrophins and ovarian drilling
When IVF may help and how clinics reduce OHSS risk
Pregnancy monitoring and frequently asked questions
Oocyt clinical principle PCOS is one part of the fertility picture. A strong treatment plan also considers age, sperm, fallopian tubes, metabolic health, treatment burden and your priorities. |
|---|
A note about the name
In May 2026, international organisations introduced polyendocrine metabolic ovarian syndrome, or PMOS, as the new name for the condition previously called polycystic ovary syndrome, or PCOS. The new name reflects that the condition affects hormones, metabolism, mental health, skin and reproduction - and is not defined by ovarian cysts. [3,4]
What is PCOS (PMOS)?
PCOS is a common hormonal and metabolic condition. It affects about one in eight women worldwide and can begin after puberty. Symptoms and severity vary widely. Some people have obvious cycle or skin symptoms; others are diagnosed during fertility investigations. [3]
Despite the old name, PCOS is not caused by ovarian cysts. The “polycystic” appearance describes a higher number of small follicles that have started developing. These follicles are usually harmless.
How is it diagnosed?
In adults, diagnosis usually requires a combination of features after other causes have been excluded. These may include irregular or absent ovulation, clinical or biochemical signs of higher androgen activity, and polycystic ovarian morphology on ultrasound or an appropriate AMH-based pathway. A scan alone is not enough to diagnose PCOS. [1]
Possible features Irregular or absent periods, acne, increased facial or body hair, scalp hair thinning, difficulty conceiving, insulin resistance, weight changes, sleep problems, anxiety or low mood. Not everyone has every feature. |
|---|
How does PCOS affect fertility?
The main fertility issue is often irregular ovulation. A follicle may begin to develop but not consistently mature and release an egg. This creates fewer predictable fertile windows and makes timing intercourse or insemination harder.

PCOS may also be linked with insulin resistance and higher androgen activity, which can affect ovulation. However, PCOS does not automatically mean low ovarian reserve. AMH can be higher because the ovaries contain more small follicles, but a high AMH result does not guarantee pregnancy or measure egg quality.
Can you get pregnant naturally? Yes. Some people with PCOS ovulate occasionally and conceive without fertility treatment. Others need support to make ovulation more regular. How long this takes depends on age, sperm, tubal health, cycle pattern and any additional fertility factors. |
|---|
How to improve your chances of pregnancy with PCOS
There is no single food plan, supplement or exercise routine that “fixes” PCOS. The aim is to build sustainable habits that support metabolic health, pregnancy health and emotional wellbeing. Benefits can occur even when body weight does not change. [1]
Folic acid and medicines
Take preconception folic acid at the dose recommended for you. Review prescribed medicines, over-the-counter products and supplements with a clinician because some may be unsuitable during pregnancy or may interact with fertility treatment.
Avoid unsupported promises “Anti-inflammatory diets”, green tea, fertility detoxes and supplement stacks are often marketed aggressively. They may be expensive and are not substitutes for a fertility assessment or evidence-based treatment. |
|---|
Weight, insulin resistance and fertility
PCOS care should not reduce your health to a number on the scale. The international guideline recommends healthy lifestyle support for everyone with PCOS, with attention to preventing weight gain and improving metabolic health. Where weight loss is personally appropriate and safe, even a modest change may help ovulation for some people, but it should not be presented as a guarantee or a condition for respectful care. [1]
Health checks worth discussing
Blood pressure
Glucose testing, often with an oral glucose tolerance test when planning pregnancy or fertility treatment
Lipids and cardiovascular risk where appropriate
Sleep apnoea symptoms
Mental health and eating-disorder risk
Folic acid dose, vaccinations and long-term conditions
Oocyt note If weight conversations have previously felt blaming or dismissive, ask for a plan focused on measurable health outcomes: ovulation, blood pressure, glucose, sleep, movement, nutrition and treatment access. |
|---|
What should be checked before fertility treatment?
It is easy to assume that PCOS explains every delay in conception. That can lead to months of treatment while another factor remains unrecognised. Assessment should match your age, history and treatment route.
A useful clinic question “Before we start ovulation treatment, have we checked whether sperm and fallopian-tube factors could change the plan?” |
|---|
How effective are fertility treatments for PCOS?
Treatment is often highly effective because the main problem - irregular ovulation - can frequently be treated. The route should be stepped, monitored and adapted to your response rather than assuming IVF is immediately necessary. Treatment success depends on more than the medicine. Age, egg quality, sperm, fallopian tubes, treatment timing and how consistently ovulation occurs all influence the chance of pregnancy and live birth.

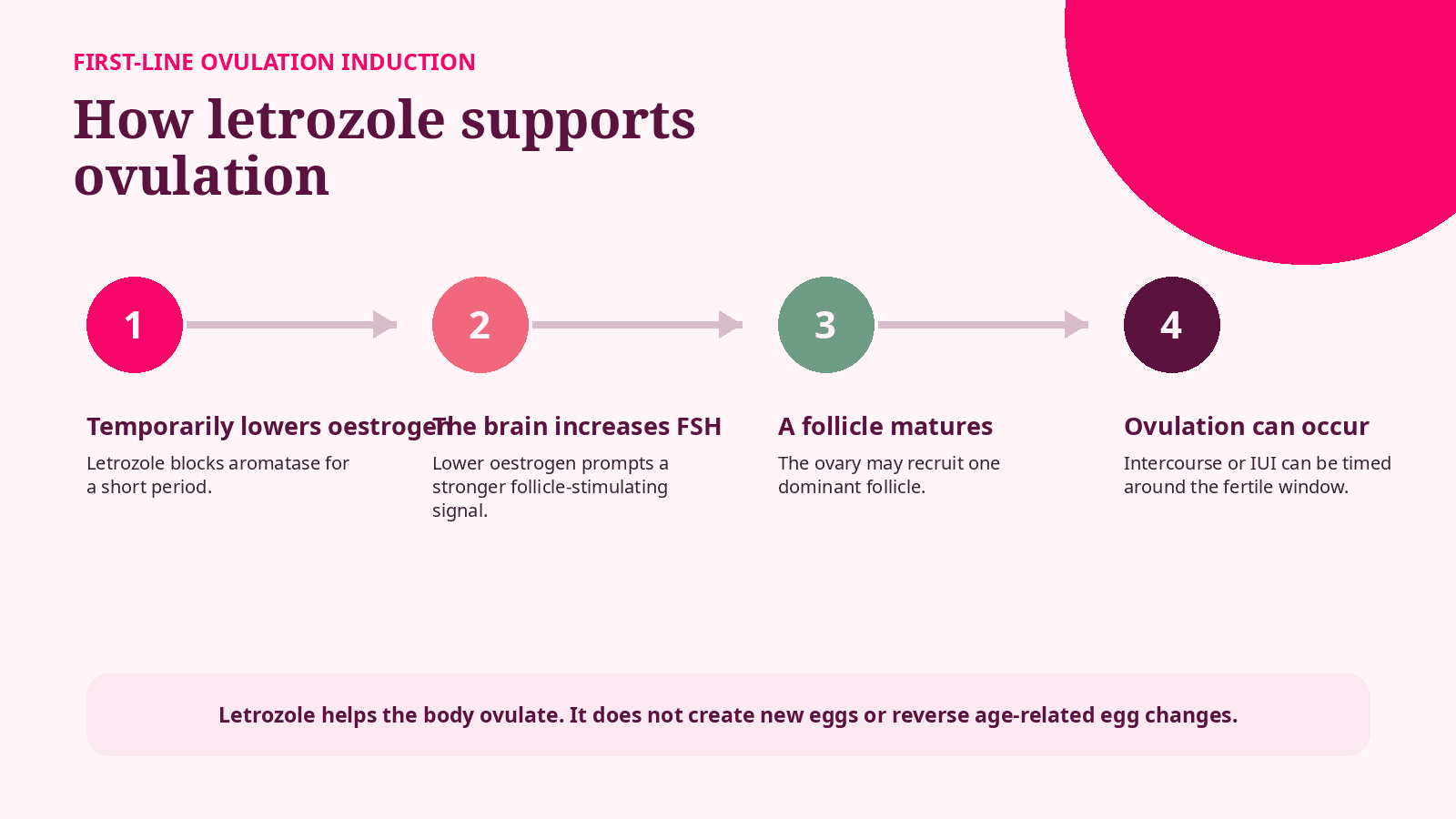
1. Letrozole: preferred first-line treatment
For anovulatory infertility caused by PCOS, letrozole is the preferred first-line fertility medicine in current international guidance. IVF can be effective, but it is usually considered after simpler treatments have not worked or when another fertility factor makes IVF the better route. [1,2]
Letrozole temporarily lowers oestrogen, prompting the brain to release more follicle-stimulating hormone. This can help one follicle mature and ovulate. The 2023 international guideline recommends letrozole as the first-line medicine for anovulatory infertility in PCOS when no other infertility factor has been identified. [1]
In the landmark trial of 750 women with anovulatory PCOS, cumulative live birth over up to five cycles was 27.5% with letrozole and 19.1% with clomiphene. This was a study-wide cumulative result, not a personal per-cycle prediction. [5]
Monitoring varies Some clinics use ultrasound in the first or selected cycles, while others use progesterone blood tests or cycle tracking. Follow the protocol given by your own fertility team and do not change the dose independently. |
|---|
Possible side effects
Hot flushes, headache or tiredness
Dizziness or muscle aches
Visual symptoms, which should be reported
More than one mature follicle and a risk of multiple pregnancy
2. Metformin and clomiphene
Metformin
Metformin improves insulin sensitivity and may support cycle regularity or ovulation in selected people with PCOS. It can be used alone or alongside other treatment, but patients should be told that more effective ovulation medicines are available for many fertility situations. Gastrointestinal side effects are common. [1]
Clomiphene citrate
Clomiphene stimulates ovulation by blocking oestrogen receptors. It remains an option, alone or with metformin in selected cases, but letrozole is generally preferred for anovulatory PCOS because it produces better ovulation, pregnancy and live-birth outcomes. [1,5]
Treatment | Where it may fit | Important point |
|---|---|---|
Letrozole | Preferred first-line medicine | Best-supported live-birth evidence in anovulatory PCOS |
Metformin | Selected metabolic or fertility situations | May be less effective alone than first-line ovulation-induction medicines |
Clomiphene | Alternative or combination option | Can affect cervical mucus or the endometrium in some patients |
Supplements Evidence for inositol and many “fertility supplements” remains uncertain. Discuss products with your clinician, especially when combining them with prescribed medication. |
|---|
3. Gonadotrophins and ovarian drilling
Gonadotrophin injections
Gonadotrophins directly stimulate follicle growth. They can work when oral medication has not produced ovulation, but they require ultrasound monitoring because multiple follicles and ovarian hyperstimulation can occur. Low-dose step-up protocols are commonly used to aim for one mature follicle.
Laparoscopic ovarian surgery
Laparoscopic ovarian drilling may be considered as a second-line option in selected people with anovulatory PCOS. During keyhole surgery, small areas of androgen-producing ovarian tissue are treated. It may restore ovulation, but it involves anaesthesia and surgery, and it is not a routine first-line treatment. [1]
Keep the goal clear The aim is not to produce as many follicles as possible. For timed intercourse or IUI, the safest target is usually a controlled response that limits the risk of twins or higher-order pregnancy. |
|---|

Can you have IVF with PCOS?
Yes. IVF can be highly effective for people with PCOS. It may be recommended after ovulation-induction treatments have not worked, or sooner if there are blocked tubes, significant sperm factors, a need for genetic testing, or another reason that makes IVF appropriate.
PCOS ovaries can produce a strong response to stimulation, which may mean a good number of eggs but also a higher risk of ovarian hyperstimulation syndrome, or OHSS. Modern protocols allow clinics to reduce this risk. [1]

The exact IVF protocol depends on age, ovarian reserve, previous response, clinic practice and treatment goals.
What affects IVF success with PCOS?
A high egg number does not automatically mean a high live-birth rate. The quality and chromosomal health of eggs are strongly influenced by age. Embryology, sperm quality, uterine factors and embryo-transfer strategy also matter.
Age at egg collection
Previous pregnancy and treatment history
Sperm quality and whether ICSI is needed
Number and maturity of eggs
Embryo development and laboratory quality
Uterine cavity and endometrial factors
Single embryo transfer and the number of treatment attempts
Ask for the right number When comparing clinic results, ask for the live-birth rate for patients of your age and treatment type. Pregnancy rates, positive tests and egg numbers are not the same as live birth. |
|---|
Pregnancy after conceiving with PCOS
Most people with PCOS who become pregnant go on to have healthy babies. However, PCOS is associated with a higher chance of gestational diabetes, high blood pressure, pre-eclampsia, miscarriage and preterm birth. This does not mean these complications will happen; it means preconception care and antenatal monitoring are important. [1]

Medication safety Do not start, stop or continue metformin, fertility medicines or supplements during pregnancy without advice from the clinician responsible for your care. |
|---|
Common PCOS fertility myths
“PCOS means I cannot get pregnant.” False. Many people conceive naturally or with treatment. |
|---|
“The follicles are dangerous cysts.” Usually false. The ultrasound appearance reflects small follicles, not the type of cyst that normally needs surgery. |
|---|
“IVF is the only option.” False for many patients. Ovulation induction is usually tried first when anovulation is the main issue. |
|---|
“High AMH means I am very fertile.” False. AMH may be high in PCOS because there are more small follicles; it does not measure egg quality. |
|---|
“If I lose weight, pregnancy is guaranteed.” False. Health improvements may support ovulation and pregnancy, but fertility is influenced by several factors. |
|---|
“Supplements can cure PCOS.” False. No supplement cures PCOS, and evidence for many products is limited. |
|---|
The emotional side of trying to conceive with PCOS
Irregular cycles can make trying to conceive feel unpredictable. Repeated tracking, pregnancy tests, weight-focused conversations and visible symptoms such as acne or hair growth can affect confidence and mood. These experiences deserve care, not dismissal.
Ask for explanations in plain language and written next steps
Set a review point for each treatment rather than repeating cycles indefinitely
Use counselling or peer support when treatment begins to dominate daily life
Discuss intimacy and relationship strain without blame
Seek help for anxiety, low mood, disordered eating or body-image distress
Frequently asked questions
How long does it take to get pregnant with PCOS?
There is no fixed timeline. Some people conceive in the first ovulatory cycles, while others need dose adjustment, additional investigation or IVF. Age and other fertility factors matter.
Can I ovulate with irregular periods?
Yes. Irregular cycles can still include occasional ovulation, but the fertile window is harder to predict.
Are ovulation predictor kits accurate with PCOS?
They can be harder to interpret because LH may be persistently elevated. Your clinic may suggest progesterone testing or ultrasound instead.
Does metformin help everyone with PCOS get pregnant?
No. It can be useful in selected people, but it is not the most effective fertility treatment for every patient.
Is IVF more risky with PCOS?
The main treatment-specific concern is a stronger ovarian response and OHSS. Individualised protocols substantially reduce this risk.
Can PCOS cause miscarriage?
PCOS is associated with an increased miscarriage risk at population level, but many people have uncomplicated pregnancies. Age and metabolic health also contribute.
Should I take inositol?
Evidence is still uncertain for fertility outcomes. Discuss the product, dose, cost and any medicines with your clinician.
When should I seek fertility help?
Seek advice after 12 months of trying if under 36 and there is no known factor. Ask earlier if aged 36 or over, periods are absent or very irregular, or there are concerns about sperm, tubes or another condition. [2]
The bottom line
PCOS can delay ovulation. It does not remove the possibility of pregnancy. A good fertility plan starts with the whole picture, uses letrozole first when appropriate, moves through treatment in measured steps, and plans IVF carefully when it becomes the right option. |
|---|
The most useful question is not simply, “Can I get pregnant with PCOS?” It is: “What is preventing pregnancy in my specific situation, and what is the safest next step?”
Considering fertility treatment? Start with clarity.
Oocyt helps you understand your options, compare fertility pathways and prepare for informed conversations with clinics locally or internationally.
Book a consultation Visit oocyt.org to speak with the Oocyt patient support team about your next steps. |
|---|
References
1. Teede, H.J. et al. (2023). Recommendations from the 2023 International Evidence-based Guideline for the Assessment and Management of Polycystic Ovary Syndrome. Journal of Clinical Endocrinology & Metabolism, 108(10), 2447-2469. https://doi.org/10.1210/clinem/dgad463
2. NICE (2026). Fertility problems: assessment and treatment. NICE guideline NG257. https://www.nice.org.uk/guidance/ng257
3. Monash University (2026). Polyendocrine Metabolic Ovarian Syndrome: new name to improve diagnosis and care. https://www.monash.edu/medicine/news/latest/2026-articles/polyendocrine-metabolic-ovarian-syndrome-new-name-to-improve-diagnosis-and-care-of-condition-affecting-170-million-women-worldwide
4. European Society of Human Reproduction and Embryology (2026). PCOS Name Change. https://www.eshre.eu/Guidelines-and-Legal/Position-statements/PCOS-Name-Change
5. Legro, R.S. et al. (2014). Letrozole versus clomiphene for infertility in the polycystic ovary syndrome. New England Journal of Medicine, 371, 119-129. https://doi.org/10.1056/NEJMoa1313517
6. NHS (2026). Polyendocrine metabolic ovarian syndrome (PMOS). https://www.nhs.uk/conditions/polyendocrine-metabolic-ovarian-syndrome-pmos/
Editorial disclaimer Oocyt provides fertility education, navigation and support services. We do not diagnose, prescribe or replace personalised medical care. Medical decisions should be made with qualified healthcare professionals and your treating clinic. |
|---|