Treatment Journeys
Amatoritsero Olumami-Oyibo ·
4 min read


PUBLISHED 15 JULY 2026 • PART 4 • OVULATION INDUCTION
Medical information, not personal medical advice Letrozole should only be used under the direction of a qualified fertility clinician. Your age, diagnosis, ovarian response, sperm results, tubal health and treatment setting all affect your individual chance of success. |
|---|
AMH and ovarian reserve
What the test can tell you about letrozole treatment - and what it cannot
Anti-Müllerian hormone, or AMH, is one of the most discussed fertility blood tests. It can be genuinely useful when planning treatment, but it is often marketed as a direct score of fertility or egg quality. That interpretation goes beyond what the evidence supports.
What is ovarian reserve?
Ovarian reserve describes the remaining pool of follicles that may be recruited as eggs mature. It is not the same as the number of eggs visible on a scan, and it is not the same as egg quality. Common measures include AMH, antral follicle count on ultrasound and, in some contexts, FSH measured early in the cycle.
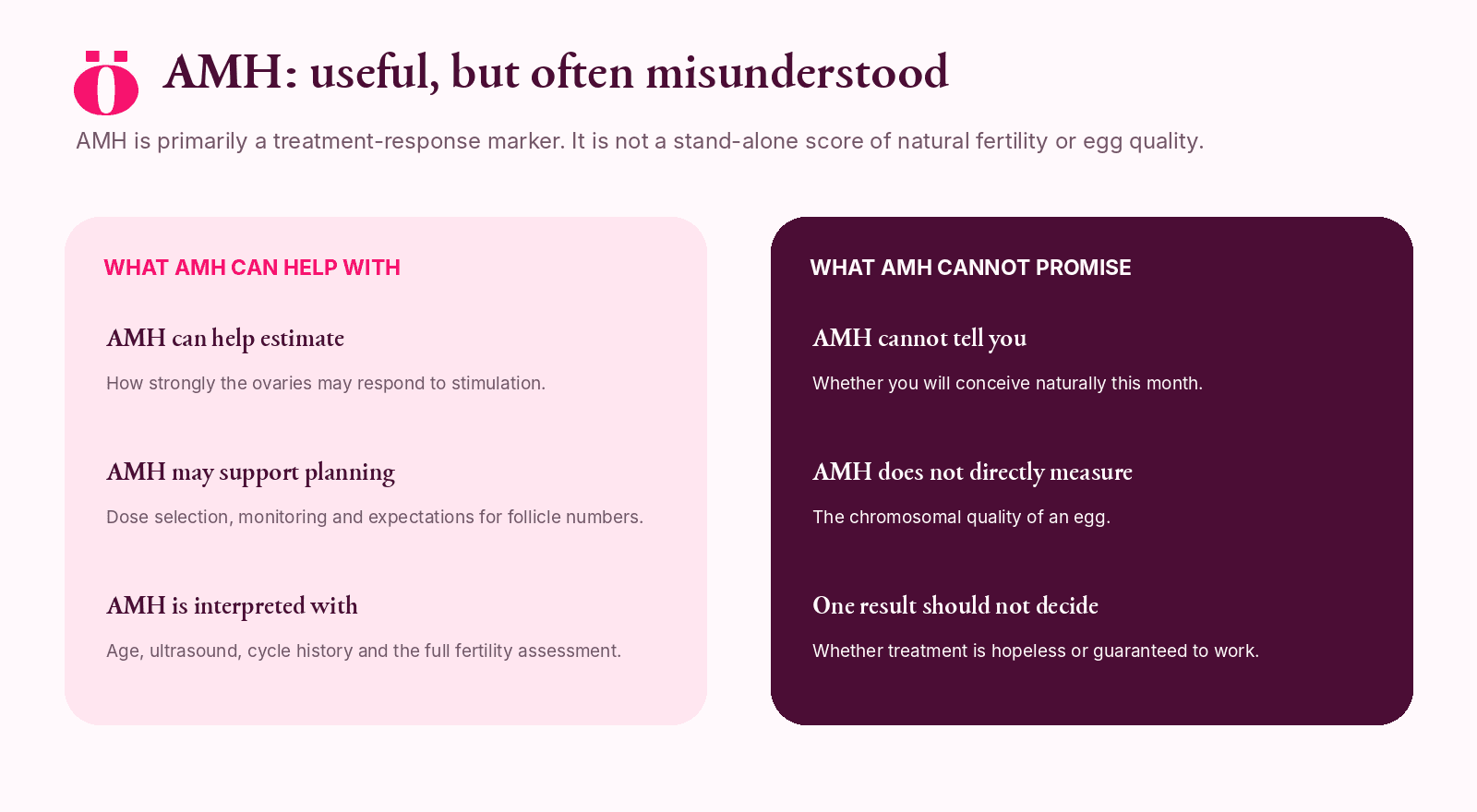
How AMH may help in a letrozole plan
It may help the clinician anticipate whether the ovaries are likely to respond weakly, typically or strongly.
It may be considered alongside ultrasound and cycle history when choosing monitoring intensity.
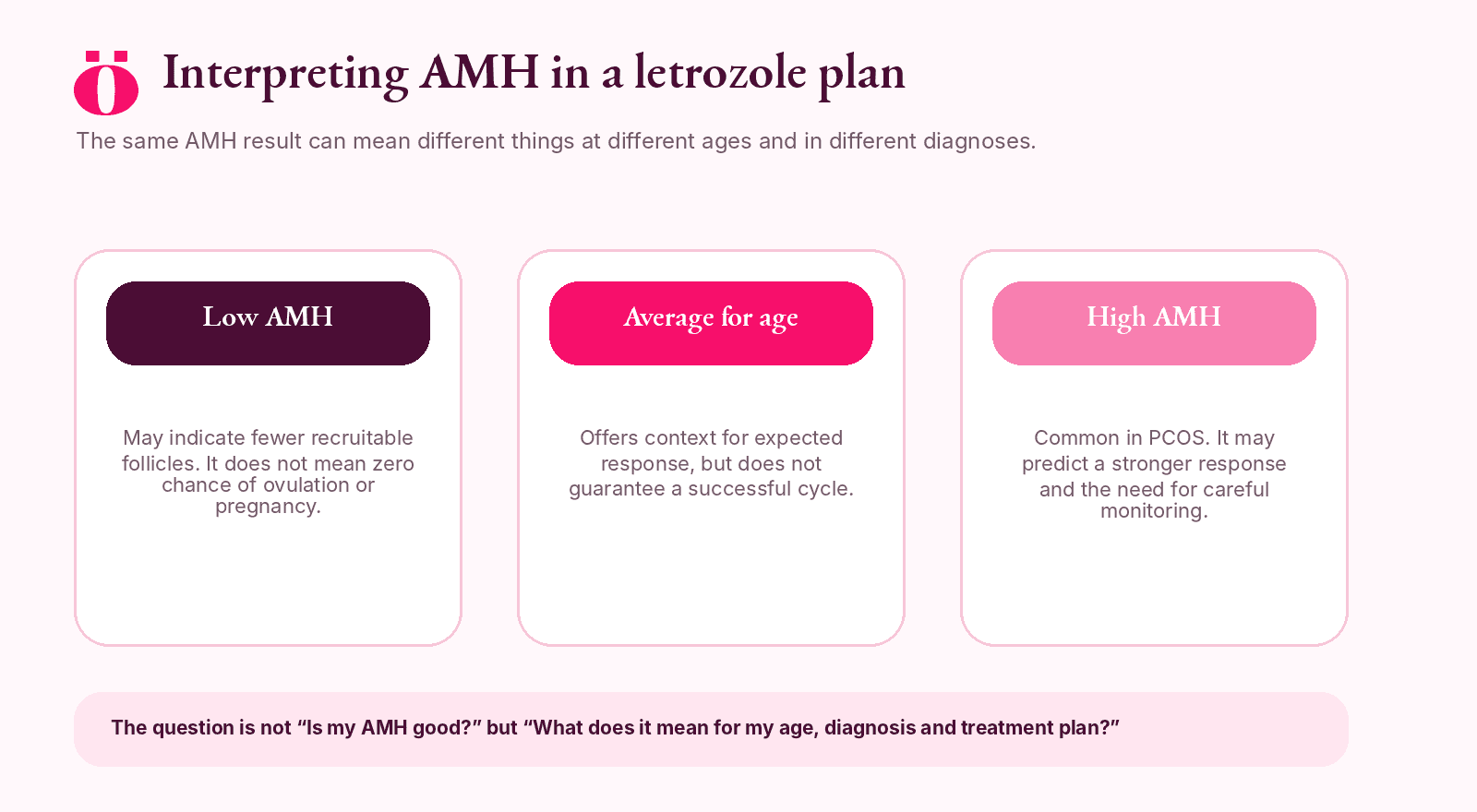
A high AMH result in PCOS may support careful dose escalation and monitoring because multiple follicles can develop.
A low AMH result may prompt a more time-sensitive review, especially when age or other fertility factors are present.
Low AMH does not mean no chance
A low AMH result may indicate that fewer follicles are available to respond. It cannot prove that no egg will mature, that ovulation induction cannot work or that natural conception is impossible. One egg may be sufficient for pregnancy, while the probability of obtaining that egg and the value of time still need realistic discussion.
High AMH does not guarantee pregnancy
AMH can be high in PCOS because many small follicles produce the hormone. This may coexist with irregular ovulation. A larger follicle pool does not automatically mean better egg quality or a higher chance of live birth. High ovarian reserve and effective ovulation are different issues.
Why age still matters more for egg quality
Two people can have similar AMH levels and very different reproductive outlooks because they are different ages. AMH is more useful for predicting the number of follicles or eggs that might respond to treatment than for predicting the chromosome health of those eggs. ASRM guidance cautions against using ovarian-reserve tests as stand-alone predictors of reproductive potential. [1]
AMH results can vary
Laboratories use different assays and reference ranges.
Hormonal contraception and some medical conditions may affect interpretation.
A single value should be considered with age, ultrasound, cycle pattern and previous treatment response.
Small numerical differences between tests may not represent a meaningful biological change.
Oocyt clinical insight Do not ask only, “Is my AMH normal?” Ask, “What does this result mean for my age, diagnosis, expected response and treatment timeline?” |
|---|
When AMH and letrozole seem to disagree
A person with low AMH may still develop a dominant follicle on letrozole. A person with high AMH may still fail to ovulate at the starting dose. The monitored response is direct evidence of what the ovaries did in that cycle, so treatment decisions should not be based on the AMH value alone.
Questions to ask after an AMH result
Is this result expected for my age and diagnosis?
How does it compare with my antral follicle count?
Does it change the starting plan or only the monitoring plan?
What would count as an adequate response to letrozole?
Does this result make treatment more time-sensitive?
When will the plan be reviewed if I ovulate but do not conceive?
The bottom line
AMH is a useful piece of a fertility assessment. It is not a verdict. Its main value is helping clinicians anticipate ovarian response and plan treatment alongside age, ultrasound, diagnosis and the wider fertility picture.
References
1. American Society for Reproductive Medicine (2020) Testing and interpreting measures of ovarian reserve: a committee opinion. Fertility and Sterility, 114(6), 1151-1157.
2. ACOG (2019) The use of antimüllerian hormone in women not seeking fertility care. Committee Opinion No. 773.
3. Teede, H.J. et al. (2023) International evidence-based guideline for the assessment and management of polycystic ovary syndrome.
4. NICE (2026) Fertility problems: assessment and treatment. NICE guideline NG257.
Editorial disclaimer Oocyt provides fertility education, guidance and support services only. We do not provide medical advice, diagnosis or treatment. Medical decisions should be made with licensed healthcare professionals and your treating clinic. |
|---|